Hello Blurt!
In today's article, I'll explore Snake Bites especially in Sub-Saharan Africa and the science behind Antivenoms. I have seen a few cases of snake bites myself. Snakes Bite 1.5 Million People in Sub-Saharan Africa Yearly. Snakebites are a significant burden in Sub-Saharan Africa.
Research has shown though that the country most heavily affected by snakebites in the world is India. According to Wikipedia,
According to the most conservative estimates, at least 81,000 snake envenomings and 11,000 fatalities occur in India each year, making it the most heavily affected country in the world.
According to one of Achebe's works of African literary realism,
May we escape danger in the farm – the bites of a snake or the sting of the scorpion… Chinua Achebe, Arrow of God. 1964
Snake Bites
Snake Bites

Snake bite injury in a 9 year old female patient from Villa de Cura, Venezuela. By Bobjgalindo - Own work, CC BY-SA 4.0, Link
What is a venomous bite?
A venomous bite is a bite or sting involving injection of a venom.
There are more than 3000 species of snakes worldwide but only about 15% are dangerous. Snakes are found worldwide apart from Antartica They can be classified into venomous and non-venomous snakes.

Map showing the approximate world distribution of snakes. By Eightofnine - Own work, Public Domain, Link
Epidemiology
Epidemiology
In Nigeria,the incidence of bites is 497/100,000 population/yr with a 12% natural mortality with the species Echis occelatus accounting for at least 66% of cases.

Map showing the global distribution of snakebite morbidity. By Eightofnine - Own work, Public Domain, Link
Snake bites affects all age groups but is commoner in males aged 11-50yrs.
The male to female ratio is 2:1.
Rural to urban ratio is 9:2.
The peak time of incidence is between 4am and 12am and 2/3rds of all bites occur in the lower limbs.
Person groups at risk of snake bites include:
- Farmers
- Herdsmen
- Plantation workers
- Herpetologists
- Snake charmers
- Campers
- Young children and elderly in Suburban areas
Classification
Classification
According to Wikipedia,
Venomous snakes are species of the suborder Serpentes that are capable of producing venom, which they use for killing prey, for defense, and to assist with digestion of their prey. The venom is typically delivered by injection using hollow or grooved fangs.
Venomous snakes can be divided into 4 main groups:
- Viperidae – Vipers and adders
- Elapidae – Mambas and cobras
- Hydrophidae – Sea snakes (commonly found in Asian-Pacific waters)
- Colubridae- Boomslang, vinesnake, twigsnake
In Nigeria, 3 main species are associated with envenomation:
- Carpet viper (Echis ocellatus)
- Black necked spitting cobra (Naja nigricollis)
- Puff adder (Bitis arietans)
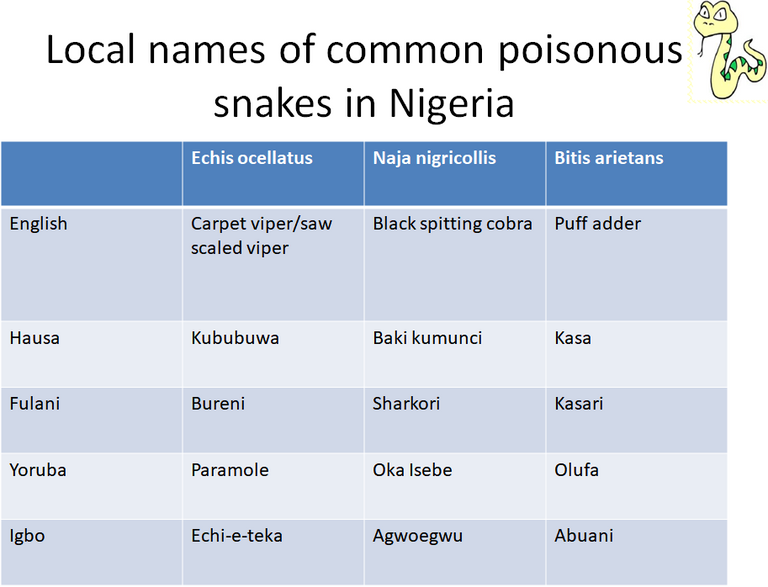
Image created by @gamsam
Echis occelatus
Echis occelatus
They has an average length of 30 to 50cm (max. 70cm). They are reddish brown/grayish snake with pale oval or rhomboidal dorsal markings connected by a dark median band and flanked by white spots ‘eyes’ bordered with black scales. The belly is white, heavily spotted with black
Echis occelatus, Nigeria © David J. Williams | Source: WHO Snake Gallery
Echis leucogaster
Echis leucogaster
They have an average length 30-70cm (max 87cm). There is an undulating pale line on the flanks which is usually incomplete, producing a series of inverted U-shaped or crescentic marks either side of the dorsal series of pale patches, which sometimes form a zig-zag pattern. The belly is pure white.
Bitis arietans (Puff Adder)
Bitis arietans (Puff Adder)
They are very large and heavy bodied snake.
They have a maximum length of over 190cm. They are usually black, brown, reddish or orange in color. They have distinctive pale black edged U or V marks along the dorsum which become annular rings around the tail.
Their bellies are pale with blackish marks.
When it is threatened, it inflates its body and hisses loudly by expelling air through its dorsally placed nostrils.
 Puff adder (Bitis arietans) head, Darmstadt Vivarium, Darmstadt, Germany. By Julius Rückert - Own picture, taken by me JuliusR, CC BY-SA 3.0, Link
Puff adder (Bitis arietans) head, Darmstadt Vivarium, Darmstadt, Germany. By Julius Rückert - Own picture, taken by me JuliusR, CC BY-SA 3.0, Link

Bitis arietans (adult). By 4028mdk09 - Own work, CC BY-SA 3.0, Link
Naja nigricollis
Naja nigricollis
They have an average length of 100-150cm and a maximum of 220cm. They are usually dark grey, black or brown with pinkish red throat bands.

A black-necked spitting cobra (Naja nigricollis) in a defensive posture. By Warren Klein, CC BY-SA 3.0, Link
Snake Venom
Snake Venom
According to ,Wikipedia
Snake venom is a highly modified saliva containing zootoxins that facilitate the immobilization and digestion of prey, and defense against threats. It is injected by unique fangs during a bite, and some species are also able to spit their venom.
The primary function of snake venom is to help the snake immobilize & eventually digest its prey. More than 90% of the dry weight is protein. The most important venom components that lead to significant clinical effects after a bite are enzymes and polypeptide toxins.
The amount of venom injected during a bite depends on various factors:
- Species and size of the snake
- Mechanical efficiency of the bite
- Whether one or two fangs penetrated the skin
- Whether there were repeated bites.
Not all bites by venomous snakes lead to envenomation. On more than 50% of cases, no venom is injected. This is called a 'Dry' bite.
Even after several bites or after eating their prey, snakes do not exhaust their venom and they remain just as venomous.
Snake Venom Composition
Snake Venom Composition
They are complex secretions which contain:
- High molecular weight enzymes(molecular weight of 13-150kDa) which form 80 to 90% of viper and 25 to 70% of elapid venoms.
- Polypeptide toxins(molecular weight of 5-10kDa).
- Low molecular weight compounds (molecular weight <1.5kDa)
The enzymes include endopeptidases and serine proteases to digest the snake’s prey.
The most important venom components that cause significant clinical effects after a bite are the enzymes and polypeptide toxins. They include:
- Procoagulant enzymes
- Cytolytic or necrotic toxins
- Haemolytic and myolytic phospholipases A2
- Pre- and post-synaptic neurotoxins and haemorrhagins
Clinical Features of Snake Bite
Clinical Features of Snake Bite
Some of the clinical presentation of venomous snake bites include:
- Overwhelming fear
- Panic
- Anxiety
- Nausea
- Vomiting
- Tachycardia
- Sweating
- Diarrhea
- Pain
- Swelling
- Bleeding

The most common symptoms of any kind of snake envenomation. By Mikael Häggström. Häggström, Mikael (2014). "Medical gallery of Mikael Häggström 2014". WikiJournal of Medicine 1 (2). DOI:10.15347/wjm/2014.008. ISSN 2002-4436. Public Domain.orBy Mikael Häggström, used with permission. - All used images are in public domain. ReferencesMedlinePlus > Snake bites From Tintinalli JE, Kelen GD, Stapcynski JS, eds. Emergency Medicine: A Comprehensive Study Guide. 6th ed. New York, NY: McGraw Hill; 2004. Update Date: 2/27/2008. Updated by: Stephen C. Acosta, MD, Department of Emergency Medicine, Portland VA Medical Center, Portland, OR. Review provided by VeriMed Healthcare Network. Also reviewed by David Zieve, MD, MHA, Medical Director, A.D.A.M., Inc. Retrieved on 19 mars, 2009Health-care-clinic.org > Snake Bite First Aid - Snakebite Retrieved on 21 mars, 2009Snake bite image example at MDconsult > Patient Education > Wounds, Cuts and Punctures, First Aid for, Public Domain, Link
{kind=link}
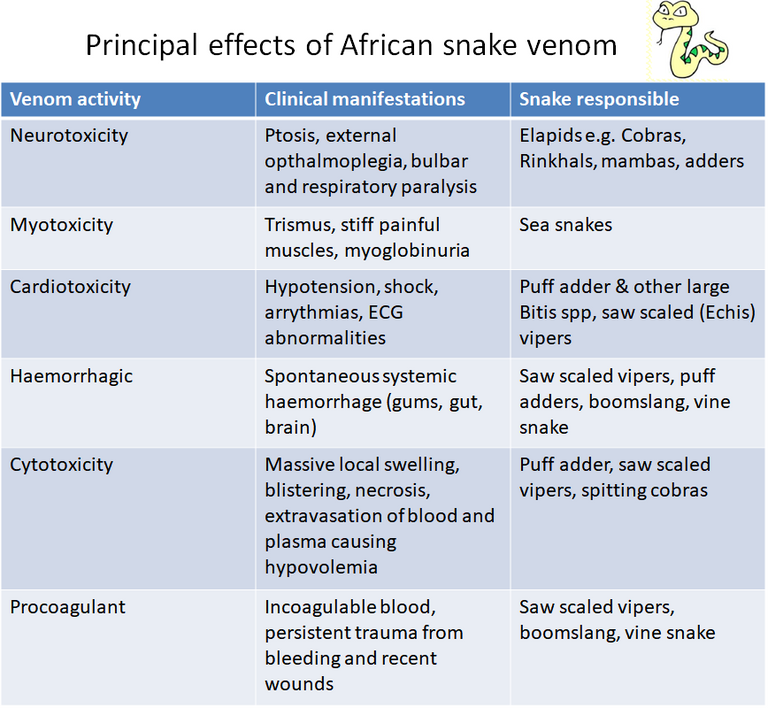
Principal effects of African snake venom. Image created by @gamsam.
Treatment
Treatment
Treatment entails:
- First Aid
- Specific therapy
- Supportive therapy
First Aid
There are certain practices associated with snake bites especially in Africa due to old traditional practices. These should be avoided. I call them the DONT'S of first aid and they include:
- Local knife/razor cuts at the site of the bite
- Attempts to suck out the venom from the wound
- Use of the black snake stone
- Use of tight tourniquets
- Electric shocks
- Application/Ingestion of herbs
What then should be done as First Aid?
- Reassure the patient - 70% of all snake bites are from non-venomous species and only 50% of bites by venomous species actually envonomate the patient.
- Immobilise the affected part with splints using bandages to stabilize. Do not make it tight so it doesn't affect the blood supply. THIS IS VERY IMPORTANT.
- Get to the hospital immediately.
- Tell the doctor of all symptoms experienced.
Pressure Immobilization
Pressure immobilization is very important but it must be done rightly or else it might cause more serious complications.
Pressure Immobilization is not appropriate for cytotoxic bites but may be effective against neurotoxic venom.
Its aim is to contain venom within a bitten limb and prevent it from moving through the lymphatic system to the vital organs.
There are two components:
- Pressure to prevent lymphatic drainage
- Immobilization of the bitten limb to prevent pumping action of skeletal muscle
An elastic bandage should be used but any cloth can be used in an emergency The bandage should be as tight as when strapping a sprained ankle. It must NOT cut off blood flow or be uncomfortable.
The location of the bite should be clearly marked on the outside of the bandages and it should be done as quickly as possible. Once applied,don’t remove till you get to a hospital. It may contain the symptoms effectively, but once removed, the venom is released into the circulation.
Identify the snake
If the snake is available, its identification can be extremely helpful.
If not available, characteristic descriptions may help eg. Cobras may rear up and spread a characteristic hood and hiss, Puff adders make a loud blowing sound,saw-scaled vipers produce a rasping sound.
Specific Therapy
The specific therapy for snake bites is the use of antivenom.
The use of antivenoms are not indicated in all situations. Antivenoms are indicated if there is:
- Hypotension
- Shock or other signs of cardiotoxicity
- Non-clotting blood
- Rhabdomyolysis
- Impaired consciousness
- Neurotoxicity – ptosis, muscle weakness,depressed respiration
- Known necrotic venom eg. Bitis arietans (puff adder)
- Swelling involving more than half of the bitten limb
- Rapid progression of swelling
- Bites on digits and into other tight fascial compartments
Antivenoms are however contraindicated in:
- Patients with an atopic history (severe asthma, hay fever etc)
- Patients with a history of previous reactions to equine antisera (eg. ATS seum) have an increased risk of severe reactions In these cases, pretreatment with SC Adrenaline and hydrocortisone is justified to prevent or diminish the reaction.
Antivenom should be given as soon as possible once signs of local or severe local envenoming are evident.
It is most effective if given within 4 hours and less effective after 8 hours. In cases of severe envenomation, it can be given even after 5 days.
Children should be given the same dose of antivenom as adults – antivenom is given to neutralize a specific dose of venom.
When patients arrive at hospital with a touniquet in place, antivenom treatment if thought necessary should be started before loosening it as there is a risk of severe envenomation when the venom in the occluded limb is released into the general circulation.
Antivenom acts only against circulating toxin, not toxin fixed to tissue and so specific measures should be taken eg. Atropine,neostigmine for neurotoxic envenomation.
There are two types of antivenom that can be used:
- Monovalent/monospecific antivenom - this is specific to only one kind of venom. It can be used if the exact species of snake that caused the bite can be reliably identified.
- Polyvalent/polyspecific - this antivenom is effective against a wide range of venoms. It is used if the species can’t be reliably identified.
Available Antivenoms in Nigeria
- South African Institute of medical Research(SAIMR) – monospecific for Echis carinatus (10-20ml)
- Fab Afrique polyvalent (40mls)
- Echilab monospecific antivenom raised against venom of Nigerian Echis occelatus
- Clomidro Costa Rican antivenom raised against venoms of 3 Nigerian snakes – Bitis arietans, Echis occelatus, Naja nigricollis (30-40ml)
Antivenom Reactions
There are some unwanted reactions or side effects associated with antivenom use. These can be classified as early or late reactions depending on how soon they occur after administration.
Early Reactions – Occur 3 to 60 minutes after administration. They include:
- Cough
- Fever
- Tachycardia
- Urticaria
- Systemic anaphylaxis
- Angioedema
Late Reactions – They occur 5 to 24 days after administration (average of 7 days). They include:
- Itching
- Urticaria
- Fever
- Arthralgia
- Proteinuria - protein in urine
- Neurological symptoms
Supportive Therapy
- Administer Tetanus toxoid to prevent Tetanus
- Use antibiotics to prevent wound infections
- Care of the bitten limb – Examine frequently for evidence of necrosis and clean with antiseptics
- Debridement of necrotic tissue – To reduce the risk of secondary infection and to promote eventual healing
- Muscle haematomas – Conservative treatment
- Amputation of doomed digits and limbs
- If there is venomous spit into the eyes, flush with large volumes of water
Prevention of Snake Bites
- Avoid walking through grass at dark when most snakes are out
- Wear heavy boots and clothes in hazardous zones
- Avoid swimming in overgrown rivers
- Avoid keeping domestic animals like chickens close to the house and ensure adequate pest control
- Avoid collecting firewood and dislodging rocks etc with bare hands
- Never put your hand into burrows or holes
- Snakes rarely attack without provocation so, avoid snakes – do not attack or disturb them.
Conclusion
Conclusion
Always try to identify a snake's distinct features after a bite as this is crucial in the treatment.
Be sure to comment below if you have any questions. I am no snake expert but we can figure it out together. 😉
Stay safe everyone, @gamsam signing out.
REFERENCES
REFERENCES
- Winkel, Ken; Kasturiratne, Anuradhani; Wickremasinghe, A. Rajitha; de Silva, Nilanthi; Gunawardena, N. Kithsiri; Pathmeswaran, Arunasalam; Premaratna, Ranjan; Savioli, Lorenzo; Lalloo, David G; de Silva, H. Janaka (2008). "The Global Burden of Snakebite: A Literature Analysis and Modelling Based on Regional Estimates of Envenoming and Deaths". PLOS Medicine. 5 (11): e218.
- Habib AG. Public health aspects of snakebite care in West Africa: perspectives from Nigeria. Journal of Venomous Animals and Toxins including Tropical Diseases [Internet]. 2013 [cited 2019 Dec 9];19(1):27. Available from: https://jvat.biomedcentral.com/articles/10.1186/1678-9199-19-27
- Habib AG, Gebi UI, Onyemelukwe GC. Snake bite in Nigeria. African Journal of Medicine and Medical Sciences [Internet]. 2001 Sep 1 [cited 2020 Jul 13];30(3):171–178. Available from: https://pubmed.ncbi.nlm.nih.gov/14510123/
- Venomous bites and stings - Clinical guidelines [Internet]. medicalguidelines.msf.org. [cited 2020 Jul 13]. Available from: https://medicalguidelines.msf.org/viewport/CG/english/venomous-bites-and-stings-18482425.html
- Wikipedia Contributors. Venomous snake [Internet]. Wikipedia. Wikimedia Foundation; 2019 [cited 2019 Nov 8]. Available from: https://en.wikipedia.org/wiki/Venomous_snake
- Snake venom [Internet]. Wikipedia. 2020 [cited 2020 Jul 13]. Available from: Bauchot R (1994). Snakes: A Natural History. New York City, NY, USA: Sterling Publishing Co., Inc. pp. 194–209. ISBN 978-1-4027-3181-5.
- Currie, Bart J.; Elizabeth Canale; Geoffrey K. Isbister (2008). "Effectiveness of pressure-immobilization first aid for snakebite requires further study". Emergency Medicine Australasia. 20 (3): 267–270(4)
- Mary Ellen Ellis. Snake Bites [Internet]. Healthline. Healthline Media; 2014. Available from: https://www.healthline.com/health/snake-bites
- Snake Bite: Symptoms, Causes, Diagnosis & Treatment [Internet]. Cleveland Clinic. [cited 2020 Jul 13]. Available from: https://my.clevelandclinic.org/health/diseases/15647-snake-bites

Written by @gamsam - a Medical Student
All images used are copyright free
Vancouver Style was used for References.
Awesome article. We have rattlesnakes here, and their venom is incredibly dangerous.