Hi everyone, how you doing?, this post is part of the previous one on trigeminal neuralgia. In this post we would discuss on the characteristics of this pain.
The character and pattern of trifacial neuralgia is as follows;
1- Severe and electric shock-like in nature.
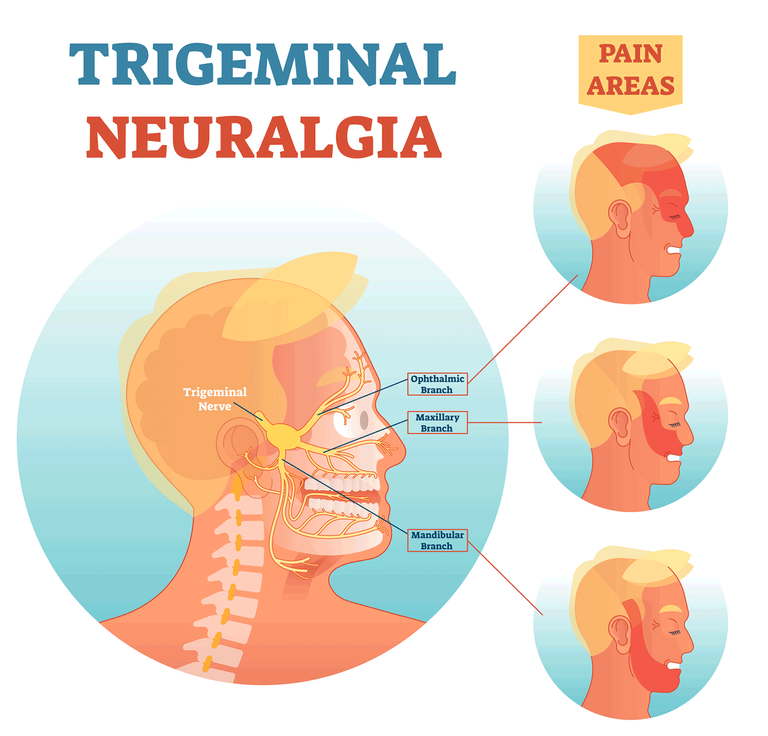
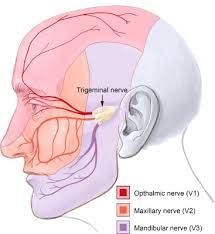
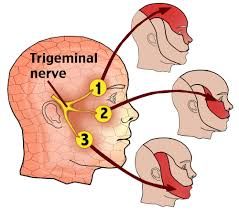
2- The pain usually occurs unilaterally along the distribution of nerve with no crossing "with no crossing the midline borders" that is rarely occur bilaterally
3- It usually occurs suddenly when triggered, last for a few seconds or minutes and disappear suddenly
4- The patient is pain-free between attacks which could range between days or years
5- The pain may occur frequently 1-2 times per day or per minute
Major points to remember as regards trifacial neuralgia;
1- It only involves the sensory involvement
2- Patient is painless and free from pain between attacks
3- Pain is usually precipitated by shaving, brushing of teeth, washing, speaking and so on.
Diagnosis of Trigeminal Neuralgia
1- History, pattern and character of pain is taken by the physician
2- Presence of trigger zones
3- Cranial nerves should be examined though it would be normal in idiopathic type of Trigeminal Neuralgia
4- Sensory and motor changes in trigeminal neuralgia disorder occurs with etiologies such multiple sclerosis, vascular malformations and brain tumour
5- Administration of local anesthesia would ward off the trigger zones during clinical examination
6- A simple tap or touch could trigger an attack during patient examination
Treatment of Trigeminal Neuralgia
Trigeminal Neuralgia as a form of Orofacial Pain could be treated both pharmacologically and surgically.
Let's begin with the pharmacologic aspect, which is the medication or drug therapy
The initial approach for TN should be the use of drugs that are effective in eliminating painful attacks (Carbamzepine, Baclofen, Gabapentin among others)
Carbamzepine
Carbamzepine is an anticonvulsant drug usually used and most effective. It is mostly used drug and has shown to be effective in treatment of more than 85% newly diagnosed cases of TN
Carbamzepine is administered slowly by increasing its doses until pain relief is achieved. The dose usually begins from the 100mg q.d.s and increased gradually to 200mg q.d.s to a maximum dose of 800mg/day.
Some patients may not respond to Carbamzepine medications alone and as such there would be a need for drug combinations or finding other substitutes
For example, Baclofen could be used as an alternative or be combined with Carbamzepine
Likewise, Gabapentin can also be added.
Side effects of Carbamzepine include
Drowsiness, vestibular disturbance, GIT upset, aplastic anemia, ataxia, loss of balance and so on
Phenytoin
Phenytoin could be used for TN when Carbamzepine is contraindicated or in addition to it in resistant cases of using Carbamzepine only
The dose of Phenytoin is 50-100mg/day then increased gradually 50mg every 2-3 days with a maximum dose of 400mg/day
Baclofen
It's analogue of gamma aminobutyric acid known GABA, which is an intrinsic inhibitory neurotransmitter
It works by lowering the presynaptic release of excitatory neurotransmitters
The dose is 50-80 mg per day in divided dose per administration.
Last but not least among the most used medications for TN is the Gabapentin.
Gabapentin
A newer anticonvulsants which is considered a first line drug for most neuropathic conditions other than the TN.
Gabapentin has fewer serious side complications like Carbamzepine and has been shown to be effective in some patients though it does not appear to be as reliable as Carbamzepine or oxcarbamazepine in efficacy.

That's all as regards this notes on trigeminal neuralgia. More would be talked about in the subsequent posts. Thanks for the usual support and attention given to the write-ups.
Happy Blogging and Reading
Video from Medical Videos YouTuber